
The evidence-based practice paper is one of the most demanding assignments in any nursing program, and the reason is not the writing difficulty. The reason is that it asks you to execute an entire research and appraisal process, write it up in academic format, and propose a clinical practice change, all in a single document. Most students are taught EBP as a concept long before they are shown how to produce the paper that proves they can apply it.
A survey published in Worldviews on Evidence-Based Nursing assessed 2,344 registered nurses across 19 hospital systems in the United States against the 24 EBP competencies established for RNs and advanced practice nurses. The finding was stark: nurses were not yet competent in any of the 24 competencies (Melnyk et al., 2018). This is not a failing on the part of those nurses. EBP is a complex skill that requires training in question formulation, systematic searching, critical appraisal, and structured academic writing. This guide covers every component of the EBP paper, from the first paragraph to the final reference, with a full worked example. For BSN and MSN students working through the appraisal, synthesis, or APA formatting stages of an EBP paper, ScribeLab Writer's nursing writing service provides support with evidence tables, clinical recommendations, and implementation plans written to Melnyk framework standards.
Quick Answer:
An EBP paper in nursing follows Melnyk and Fineout-Overholt's seven-step process. It opens with a clinical problem and its significance, formulates a PICOT question, describes the literature search methodology, critically appraises the retrieved evidence using a levels-of-evidence table, synthesizes findings into clinical recommendations, proposes an implementation plan with a named change model, describes how outcomes will be evaluated, and ends with a conclusion and dissemination plan. APA 7th edition is the required format for most US programs. Student papers do not require a running head unless the instructor specifies otherwise.
What Is an EBP Paper and Why Does Your Program Require It?
Evidence-based practice in nursing is defined as the conscientious, explicit, and judicious use of the best available evidence, combined with clinical expertise and patient values, to guide nursing decisions (Sackett et al., 1996). In nursing, Melnyk and Fineout-Overholt expanded Sackett's original clinical medicine framing into a seven-step process specifically designed for nursing practice, published across multiple editions of their landmark textbook Evidence-Based Practice in Nursing and Healthcare: A Guide to Best Practice (5th ed., 2023, Wolters Kluwer).
The EBP paper is the academic assignment through which you demonstrate that you can execute this process independently. It is not a literature review, a research proposal, or a reflective essay, although it borrows elements from each. Its distinguishing feature is that it moves through an explicit clinical question, an evidence search and appraisal, and a practice recommendation, grounded in the nursing literature.
The IOM Roundtable on Evidence-Based Medicine set a goal in 2007 that, by 2020, 90% of clinical decisions would be supported by accurate, timely, and up-to-date clinical information and reflect the best available evidence (Institute of Medicine Roundtable on Evidence-Based Medicine, 2007). That goal has not been fully realized, and the gap between research evidence and clinical practice remains a documented challenge. Your EBP paper is training for exactly that gap.
EBP Paper vs. Research Paper vs. Quality Improvement Report
Students consistently confuse these three document types. The table below shows the key differences.
Table 1: EBP Paper vs. Research Paper vs. Quality Improvement Report
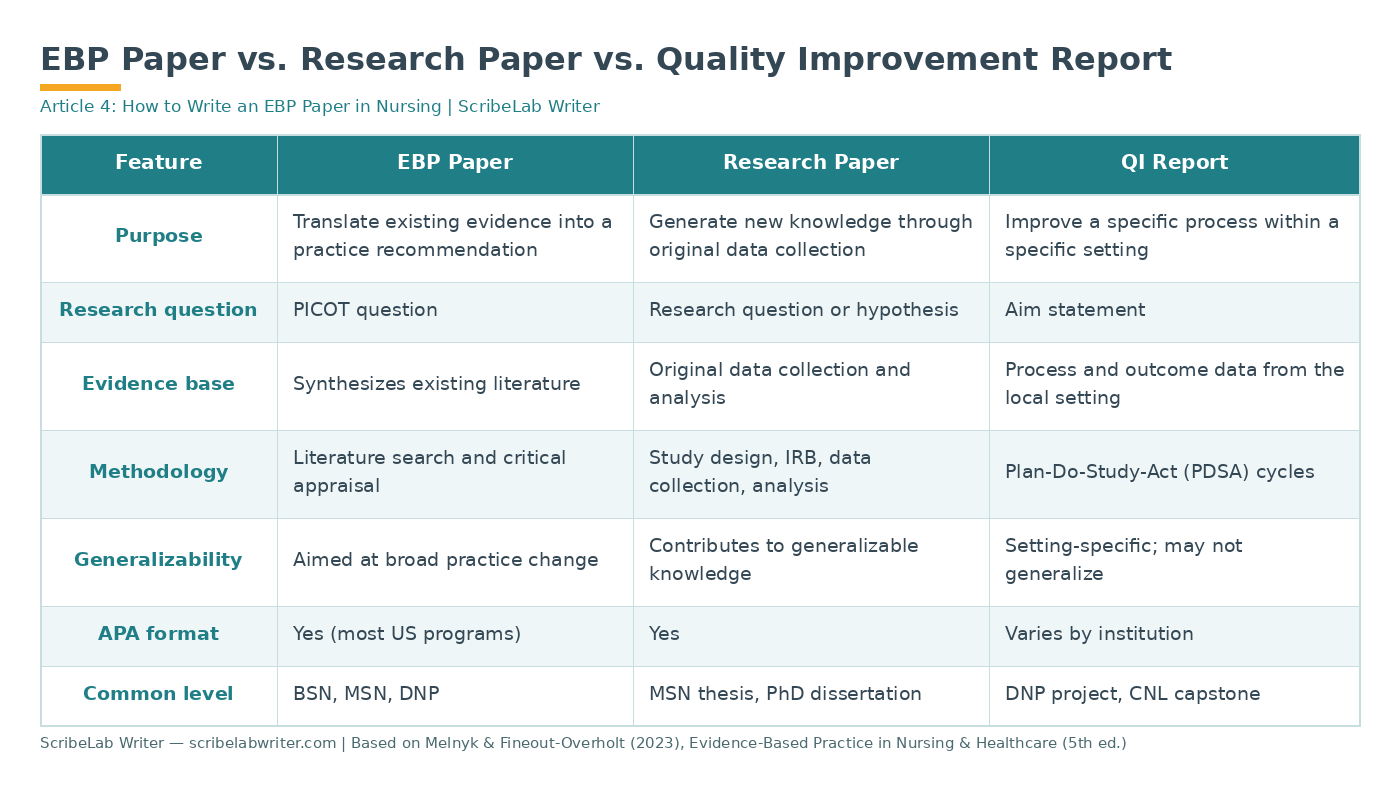
The most common mistake is submitting an EBP paper that reads like a literature review: it reviews sources but never reaches a practice recommendation. The EBP paper must end with a clear, evidence-grounded answer to the clinical question.
The Seven-Step EBP Process
Melnyk and Fineout-Overholt's seven steps, described in the 5th edition of their textbook (2023), begin with Step 0, an orientation step that precedes the formal process.
Step 0: Cultivate and sustain a spirit of inquiry. This is the professional mindset, the ongoing curiosity about whether the best evidence supports current practice.
Step 1: Ask the clinical question in PICOT format. Every EBP paper begins here. The PICOT question defines exactly what you are investigating.
Step 2: Search for and collect the most relevant best evidence. This means a systematic database search using CINAHL, PubMed, the Cochrane Library, and other appropriate databases.
Step 3: Critically appraise the evidence. Each retrieved study is evaluated for validity, reliability, and applicability to the clinical question. This is typically presented as a rapid critical appraisal using a structured tool.
Step 4: Integrate the best evidence with clinical expertise and patient preferences and values. The evidence does not stand alone; it is weighed alongside what you know as a clinician and what the patient values.
Step 5: Evaluate the outcomes of the practice decision or change. After implementation (or as part of the proposed evaluation plan in the paper), outcomes are measured against the goals.
Step 6: Disseminate the outcomes of the EBP decision or change. Sharing results, including a poster, a journal article, a staff presentation, or a policy document, completes the cycle.
Your EBP paper maps directly onto these steps. Each section of the paper corresponds to one or more steps in this sequence.
How to Structure an EBP Paper: Section by Section
The structure below represents the consensus format across major US nursing programs and reflects the Melnyk/Johns Hopkins frameworks. Your program rubric takes precedence if it specifies a different order or naming convention.
Title Page and Abstract
For student papers in APA 7th edition, the title page includes: the paper title in bold and centered, your name, the institutional affiliation, the course number and name, the instructor's name, and the due date. A running head is not required for student papers unless your instructor specifies otherwise. This is a change from the APA 6th edition that many students and instructors still miss (American Psychological Association, 2020).
An abstract is also not required for student papers in APA 7 by default, but many nursing faculty require one. If required, it runs 150-250 words, is not indented, and appears on its own page after the title page.
Introduction and Clinical Problem
This section does three things: it introduces the clinical problem, establishes its significance with specific data, and justifies the appropriateness of a nursing-led EBP inquiry.
Weak introductions state the problem in general terms ("falls are a serious issue in hospitals"). Strong introductions quantify it specifically: "The Agency for Healthcare Research and Quality estimates that between 700,000 and 1,000,000 patients fall in United States hospitals each year, with 30 to 35 percent of those falls resulting in injury" (AHRQ, 2019). The difference is the difference between a paragraph a reader can act on and one they cannot.
The introduction should also establish your professional practice context: the setting, the patient population, and why you, as a nursing professional, have identified this clinical problem.
PICOT Question
The PICOT question is the formal statement of what you are investigating. Every subsequent section of the paper must relate to it. A full guide to formulating your PICOT question is available with 15 worked clinical examples.
The PICOT question follows the format: "In [P], does [I] compared to [C] affect [O] within [T]?"
State the PICOT question explicitly in its own paragraph. Do not bury it in prose. Many faculty grade this section separately and need to see it clearly labeled.
Literature Search Methodology
This section describes exactly how you searched for evidence. It needs to be reproducible, meaning another nurse should be able to follow your described method and find the same sources. Cover four elements:
Databases searched: Name every database you used (CINAHL Complete, PubMed/MEDLINE, Cochrane Library, PsycINFO if relevant). CINAHL Complete indexes more than 5,000 nursing and allied health journals and is the primary database for nursing-specific evidence (EBSCO Information Services, 2024). PubMed provides access to over 37 million biomedical and life science citations maintained by the National Library of Medicine.
Search terms and Boolean operators: List the exact terms you used for each PICOT component and how you combined them (AND, OR, NOT). Include truncation symbols where used.
Limiters applied: Publication date range (most programs require the last 5 to 7 years), peer-reviewed only, English language, human subjects.
Results: Number of initial results, how many were excluded at the title and abstract screening stage, and how many full texts were retrieved and reviewed. This demonstrates rigor.
For guidance on confirming whether a source qualifies as peer-reviewed, see the guide on identifying peer-reviewed sources.
Evidence Review and Critical Appraisal Table
This is the analytical core of the paper. You present each included study in an evidence or synthesis table that captures: author and year, study design, sample (n and characteristics), key findings, level of evidence, and limitations.
The levels of evidence hierarchy most commonly used in US nursing programs is the seven-level framework described by Melnyk and Fineout-Overholt (2023):
Table 2: Levels of Evidence
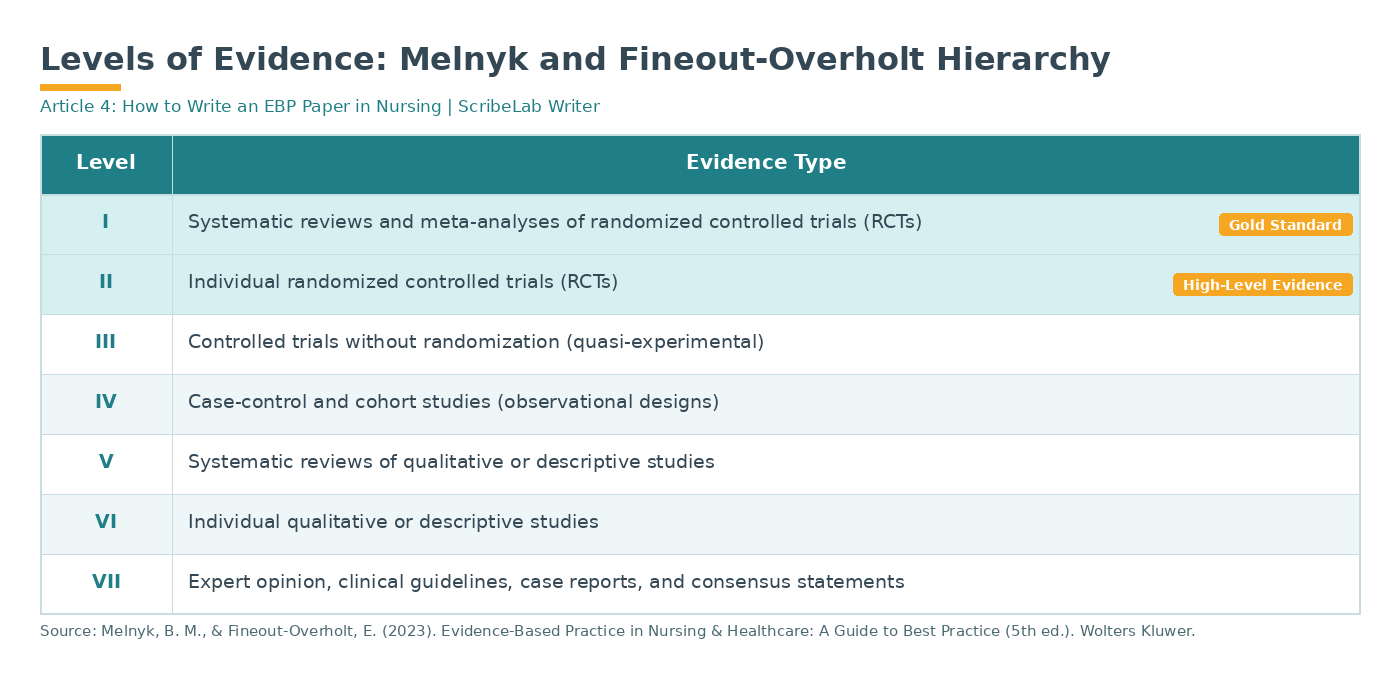
Following the table, write a narrative synthesis: summarize what the body of evidence shows across your included studies, note where evidence is consistent, where it is conflicting, and what the overall strength of the evidence is. This narrative is what distinguishes a strong EBP paper from a list of summaries.
Working on your evidence appraisal table or clinical recommendations section? |
|---|
Completing a levels-of-evidence table, appraising each study for validity and applicability, writing a narrative synthesis across multiple studies, and translating that synthesis into specific evidence-graded clinical recommendations are four distinct analytical tasks the EBP paper requires in close succession. ScribeLab Writer's nursing writing team supports BSN and MSN students with evidence appraisal tables, synthesis narratives, and clinical recommendations written to APA 7 and Melnyk framework standards. |
Discussion and Clinical Recommendations
This section answers the PICOT question directly. Based on the synthesized evidence, what should nursing practice look like? Write a clear, specific recommendation: not "the evidence suggests further research is needed" but "the evidence supports implementing a nurse-led structured hourly rounding protocol in adult inpatient units as a strategy to reduce fall rates, with strong support from two RCTs (Level II) and one systematic review (Level I)."
Connect each recommendation to a specific level of evidence. Your readers: faculty, clinicians, or future policy stakeholders: need to see that your recommendations are evidence-graded, not opinion-based.
Implementation Plan and Change Model
An EBP paper at the BSN level typically requires a brief implementation plan that names a specific change model. Three models are most commonly used:
The Iowa Model (2017) is a practical, cyclical model designed for point-of-care EBP decisions. It begins with identifying a clinical trigger: a problem or knowledge-focused trigger, and guides teams through assembling evidence, piloting a change, and evaluating outcomes (Iowa Model Collaborative, 2017). The Iowa Model is particularly well-suited for unit-level practice changes.
The Johns Hopkins Nursing EBP Model (Newhouse et al., 2007) uses a PET process: Practice question, Evidence, Translation. It provides a structured tool for appraising and rating evidence that many BSN programs use alongside the model itself.
The ACE Star Model (Stevens, 2004) describes five stages of knowledge transformation: Discovery, Evidence Summary, Translation, Integration, and Evaluation. It is particularly useful for understanding how research knowledge becomes practice knowledge.
Choose the model that best fits your clinical problem and is recommended by your program. Name it explicitly, explain why it is appropriate for your context, and map your proposed steps onto its stages.
Evaluation of Outcomes
Describe how you would measure whether the proposed practice change achieved the expected outcomes. Use the same outcome measure from your PICOT question. Name a validated measurement tool where one exists: for example, the Morse Fall Scale for fall risk, the Numeric Rating Scale for pain, or HbA1c percentage for glycemic control.
Specify the measurement frequency, who would collect the data, and what threshold would constitute a successful outcome. "Falls will decrease" is not evaluable. "A 20% reduction in falls per 1,000 patient days over 90 days, measured by the unit incident reporting system and compared to the 12-month pre-implementation baseline" is evaluable.
Conclusion and Dissemination
The conclusion summarizes the evidence, restates the clinical recommendation, and describes how findings would be disseminated. Common dissemination strategies include a unit staff presentation, a policy memo, a poster for a nursing conference, or a submission to a nursing journal.
Dissemination is Step 6 of Melnyk and Fineout-Overholt's process and is a required component of a complete EBP paper at most programs. Do not omit it.
References
All references are formatted in APA 7th edition. See the APA formatting section below for specifics on nursing-relevant source types.
Levels of Evidence in Your EBP Paper
The most important rule is this: the higher the level of evidence supporting your recommendation, the stronger the recommendation. A recommendation grounded in two Level I systematic reviews carries far more weight than one grounded in three Level VI individual qualitative studies.
If your literature search returns only lower-level evidence, acknowledge this explicitly in the discussion. A strong EBP paper does not hide weak evidence: it acknowledges the limitation and recommends generating higher-quality evidence before widespread implementation.
For the evidence table, always state the level next to each study. Do not make the reader infer it.
You May Also Find Useful
APA 7th Edition Formatting for Nursing EBP Papers
The following APA 7 requirements are the ones most commonly misapplied in nursing EBP papers.
Running head: Not required for student papers. If your faculty requires it, place it flush left in the page header on every page, in all capitals, with the page number flush right.
Title page: For student papers, include: title (bold, centered, upper and lower case), author name, institutional affiliation, course number and name, instructor name, and assignment due date. No author note.
Headings: APA 7 uses five heading levels. For a standard BSN EBP paper, you will typically use Level 1 (bold, centered, upper and lower case), Level 2 (bold, left-aligned, upper and lower case), and Level 3 (bold italic, left-aligned, upper and lower case).
In-text citations: Author (year) format for narrative citations; (Author, year) for parenthetical. For direct quotes, add the page number: (Melnyk et al., 2023, p. 14). For sources without page numbers, use paragraph number: (AHRQ, 2019, para. 3).
How to cite nursing-specific sources in APA 7:
Clinical guideline (government/organization): Agency for Healthcare Research and Quality. (2019). Preventing falls in hospitals. https://www.ahrq.gov/falls
NANDA-I: Herdman, T. H., Kamitsuru, S., & Lopes, C. T. (Eds.). (2024). NANDA international nursing diagnoses: Definitions and classification, 2024–2026 (13th ed.). Thieme.
Cochrane Review: Author, A. A., & Author, B. B. (Year). Title of review. Cochrane Database of Systematic Reviews, (issue), Article CD000000. https://doi.org/xxxxx
Nursing textbook: Melnyk, B. M., & Fineout-Overholt, E. (2023). Evidence-based practice in nursing and healthcare: A guide to best practice (5th ed.). Wolters Kluwer.
ANA Standards: American Nurses Association. (2021). Nursing: Scope and standards of practice (4th ed.). ANA.
Double spacing applies throughout, including the reference list. One-inch margins on all sides. 12-pt Times New Roman, 11-pt Calibri, or 11-pt Arial are the APA 7-approved fonts.
A Worked EBP Paper Example: Hand Hygiene and Healthcare-Associated Infections
The following condensed example demonstrates how each section connects.
Clinical problem: Healthcare-associated infections (HAIs) affect approximately 1 in 31 hospitalized patients on any given day in the United States (Centers for Disease Control and Prevention, 2024). Hand hygiene is the single most effective intervention to prevent HAI transmission. Yet, compliance rates in acute care settings consistently fall below the 80-90 percent threshold recommended by the World Health Organization.
PICOT question: In adult patients admitted to acute care inpatient units (P), does a structured nurse-led hand hygiene monitoring and feedback program (I), compared to standard hand hygiene reminders without structured monitoring (C), reduce the rate of healthcare-associated infections per 1,000 patient days (O) over a six-month period (T)?
Search methodology: Databases searched: CINAHL Complete, PubMed. Search terms: "hand hygiene compliance" AND "healthcare-associated infections" AND "nurses." Limiters: 2018 to 2024, peer-reviewed, English, human. Initial results: 142 records. After title/abstract screening: 18 full texts retrieved. After full-text review: 9 studies included (1 systematic review, 3 RCTs, 3 quasi-experimental studies, 2 cohort studies).
Evidence synthesis: The included systematic review (Level I) found that multimodal hand hygiene interventions, combining observation, feedback, and reminders, reduced HAI rates by 28 to 36 percent compared to single-component interventions. Two of the three RCTs (Level II) found statistically significant reductions in HAI rates when nurses received individualized monthly feedback on observed compliance. One quasi-experimental study (Level III) found a 22 percent increase in compliance following unit-based champion programs.
Recommendation: Implement a nurse-led multimodal hand hygiene program on the adult acute care unit consisting of monthly direct observation by a trained observer, individualized feedback to each nurse on compliance rates, and a visible unit compliance dashboard updated weekly. The evidence base includes one Level I systematic review and two Level II RCTs supporting this recommendation.
Implementation plan (Iowa Model): Identify the practice trigger (HAI rate above hospital benchmark). Assemble an EBP team (infection control nurse, unit champion, nursing manager). Pilot the program on two units over 90 days. Evaluate HAI rates against baseline. If results support practice change, roll out to all adult inpatient units and develop a policy update.
Evaluation: HAI rate per 1,000 patient days, measured monthly using the hospital infection control database. Target: 25 percent reduction from baseline at 90 days.
Common EBP Paper Mistakes
Writing a literature review instead of an EBP paper. A literature review summarizes sources. An EBP paper synthesizes evidence and reaches a practice recommendation. If your paper ends without a clear, specific recommendation and an implementation plan, it is not an EBP paper.
Using a medical diagnosis as the clinical problem. The clinical problem in an EBP paper must be one that nursing can address through nursing interventions. "What is the best treatment for sepsis?" is a medical question. "In ICU patients with early sepsis, does a nurse-led sepsis bundle monitoring protocol compared to standard nursing assessment improve time to antibiotic administration?" is a nursing question.
Not identifying the level of evidence for each study. Every study in your evidence table must have a level of evidence assigned. Do not group studies by theme without first establishing their methodological strength.
Choosing a change model without explaining why. Naming the Iowa Model without explaining why it fits your context scores poorly. Show that you understand what the model asks you to do and why it is appropriate for a unit-level practice change.
Omitting dissemination. Step 6 of Melnyk and Fineout-Overholt's process is dissemination, and it is a required section at most programs. Leave it out and you lose marks regardless of the strength of the rest of the paper.
Confusing the abstract with the introduction. The abstract is a standalone summary of the entire paper. The introduction is the opening section of the paper itself. They are not interchangeable.
How EBP Papers Are Taught Across Nursing Education Systems
United States: EBP papers are required across BSN, MSN, and DNP programs. The AACN Essentials (2021) embed EBP across all 10 domains of professional nursing education. BSN programs typically require a single EBP paper as a capstone or advanced clinical practice assignment. MSN programs require more comprehensive synthesis at the graduate level. DNP programs require the entire DNP project to be grounded in EBP.
United Kingdom: The NMC Standards of Proficiency for Registered Nurses (2018) require competency in evidence-based practice. UK programs are less likely to explicitly prescribe the PICOT/ADPIE framework, but the expectation for evidence synthesis and clinical reasoning remains the same.
Australia: NMBA Registered Nurse Standards for Practice (2016) require evidence-based care. Australian programs at the University of Sydney, the University of Melbourne, and Monash teach EBP using a mix of the Melnyk and Johns Hopkins frameworks.
Saudi Arabia and UAE: Nursing programs aligned with US accreditation standards (SCFHS, CAA) increasingly teach the Melnyk framework. EBP papers are a formal graduation requirement in many BSN programs at institutions following US curriculum models.
Frequently Asked Questions About Nursing EBP Papers
How long should a nursing EBP paper be?
Most BSN programs require 10 to 15 pages, excluding the title page and reference list. MSN programs typically require 15 to 25 pages. The exact length depends on your rubric. Do not pad to reach a page count: every section should earn its place by advancing the argument.
Can I use qualitative studies in an EBP paper?
Yes. Qualitative studies are Level V or VI in the Melnyk hierarchy. They are appropriate when your clinical question involves patient experience, barriers to care, or the meaning of a health phenomenon. If you use qualitative studies, be explicit about their level of evidence and acknowledge the limitation that they cannot provide the same strength of causal evidence as RCTs.
What is the difference between evidence synthesis and a literature review?
A literature review describes sources. Evidence synthesis analyzes and integrates what multiple sources collectively say about a clinical question. In a literature review, you might write: "Smith and Jones (2022) found that hourly rounding reduced falls." In evidence synthesis, you write: "Across three RCTs and one systematic review, hourly rounding consistently reduced fall rates by 15 to 30 percent, with effect sizes that were statistically significant in two of the four studies: a finding that supports a strong Level I recommendation."
Do I need to use a formal critical appraisal tool?
Many programs require you to use a formal tool such as the CASP (Critical Appraisal Skills Program) checklists, the Johns Hopkins Research Evidence Appraisal Tool, or the Melnyk Rapid Critical Appraisal checklists. Check your assignment guidelines. Even when a specific tool is not required, your appraisal should address the validity, reliability, and applicability of each source.
Can I write an EBP paper on a topic I chose myself?
Most programs allow students to choose a topic within the parameters set by the faculty. The topic must be a nursing-addressable clinical problem, and you must be able to retrieve sufficient peer-reviewed evidence from the last five to seven years. Topics with very recent emergence or very narrow focus may not have enough Level I or II evidence to support a strong paper.
How do I know when I have enough evidence?
The quality of evidence matters more than the quantity. Two Level I systematic reviews provide stronger support than ten Level VI opinion papers. A general guide: for BSN programs, six to ten peer-reviewed sources at Level I through IV are typically sufficient for a strong paper. For MSN, 10 to 15 sources at Level I through III. For DNP, a comprehensive search with formal inclusion/exclusion criteria and a documented PRISMA-style flowchart is expected.
What is a clinical practice guideline, and how do I cite it?
A clinical practice guideline is a systematic review of evidence plus a set of recommendations developed by a professional organization for clinical decision-making. Examples include CDC infection control guidelines, AHA cardiac care guidelines, and NICE guidelines. They are cited as organizational authors in APA 7. Use the organization name as the author and include the URL or DOI.
Writing the EBP Paper That Gets Graded Well
The EBP paper tests your ability to close the gap between what research shows and what nurses do at the bedside. The most important shift is from thinking about sources to thinking about evidence: not "what does this study say?" but "what does the collective body of evidence tell me to recommend, and how confident should I be in that recommendation?"
Follow the seven steps. Build a reproducible search. Appraise every source for level and quality. Synthesize rather than summarize. Reach a specific recommendation. Propose a realistic implementation plan with a named model. Specify how you would measure success. Disseminate the results.
If you are working with a complex clinical question or need support with the evidence appraisal, synthesis table, or APA formatting, ScribeLab Writer's nursing writing service works with BSN and MSN students across the US, UK, Australia, UAE, and Saudi Arabia.
