
A nursing care plan is a structured, written document that uses the five-step nursing process to guide individualized patient care. To write one, you follow the ADPIE framework: Assess the patient and collect data, write a NANDA-I nursing diagnosis using the PES format (Problem, Etiology, Signs and Symptoms), set measurable goals and expected outcomes, plan and implement specific nursing interventions with evidence-based rationales, and evaluate whether the goals were met.
That is the core process. In practice, the difference between a care plan that earns top marks and one that gets returned for revisions almost always comes down to three things: writing a proper nursing diagnosis instead of a medical diagnosis, setting genuinely measurable goals, and providing rationales for every intervention. This guide covers each step in detail, with 10 fully worked care plan examples across different clinical scenarios. For nursing students who need support with NANDA-I diagnosis formulation, SMART goal writing, or evidence-based rationales, ScribeLab Writer's nursing writing service works with BSN students on care plan assignments across all clinical scenarios.
Quick Answer:
A nursing care plan follows the five-step ADPIE framework. Assess the patient and collect subjective and objective data. Write a NANDA-I nursing diagnosis in PES format: [Diagnostic Label] related to [Etiology] as evidenced by [Signs and Symptoms]. Set SMART goals with a measurable indicator and a specific timeframe. Implement nursing interventions with an evidence-based rationale for each. Evaluate whether each goal was met, partially met, or not met, and revise the plan accordingly. The most common reasons care plans are returned are using a medical diagnosis instead of a nursing diagnosis and writing goals that are not measurable.
What Is a Nursing Care Plan?
A nursing care plan is the formal document through which a registered nurse applies the nursing process to an individual patient. It translates assessment findings into a structured plan of action that can be communicated across the care team, evaluated at defined intervals, and revised as the patient's condition changes.
The American Nurses Association (ANA) recognizes the nursing process as the foundation of professional nursing practice, defined through the ANA Standards of Professional Nursing Practice. The nursing process is a five-step, cyclical, critical-thinking model: Assessment, Diagnosis, Planning, Implementation, and Evaluation. Ida Jean Orlando is widely credited with originating the concept of the nursing process in 1958, and the ANA formally adopted the model in the 1970s.
In nursing education, the care plan is the primary method through which students demonstrate their ability to think clinically, connect theory to practice, and document patient-centered care. BSN programs in the US, UK, and Australia all require care plan assignments, though the specific frameworks and terminology vary across countries.
The ADPIE Framework Explained
ADPIE is the acronym for the five stages of the nursing process. Every nursing care plan follows this sequence, and every section of the care plan maps to one of these stages.
Table 1: The ADPIE Framework
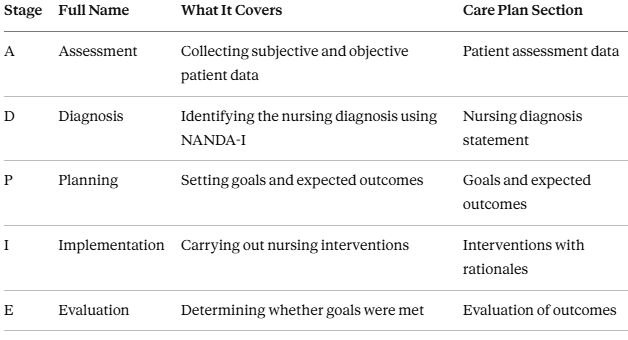
The process is cyclical. If the evaluation shows that a goal was not met or was only partially met, the nurse returns to the assessment stage, collects updated data, and revises the care plan accordingly.
What Is a NANDA-I Nursing Diagnosis?
NANDA International (NANDA-I) is the organization that develops, reviews, and publishes the standardized classification of nursing diagnoses used worldwide. The current edition is NANDA International Nursing Diagnoses: Definitions and Classification, 2024 to 2026, 13th edition, edited by T. Heather Herdman, Shigemi Kamitsuru, and Camila Takao Lopes (Thieme, 2024). This edition contains 277 nursing diagnoses organized into 13 domains and 47 classes.
A nursing diagnosis is fundamentally different from a medical diagnosis. A medical diagnosis identifies a disease or pathology and is the physician's domain. A nursing diagnosis identifies the patient's human response to an actual or potential health problem and is the nurse's autonomous domain.
Table 2: Medical Diagnosis vs. Nursing Diagnosis
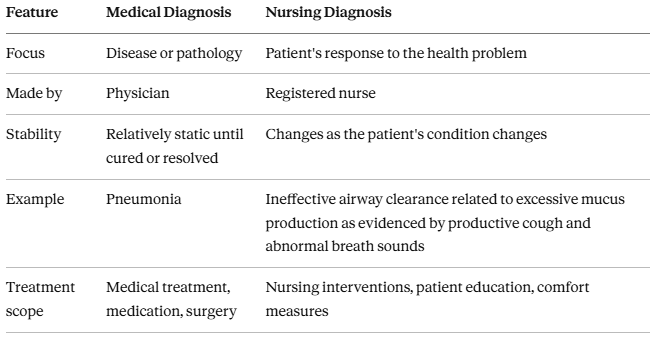
The most common mistake nursing students make is writing a medical diagnosis when a nursing diagnosis should be. "Diabetes" is a medical diagnosis. "Deficient knowledge related to newly diagnosed type 2 diabetes, as evidenced by the patient's inability to describe insulin administration technique and verbalized confusion about dietary modifications," is a nursing diagnosis.
How to Write a Nursing Diagnosis Using PES Format
The PES format is the standard structure for writing a nursing diagnosis statement. Each component maps directly to the NANDA-I diagnostic structure.
P — Problem (Diagnostic Label): The NANDA-I-approved diagnostic label that names the patient's response. Examples: Acute Pain, Risk for Falls, Ineffective Airway Clearance, Anxiety, Deficient Knowledge.
E — Etiology (Related Factors): The cause or contributing factor linked to the diagnosis, introduced by the phrase "related to." This must be something the nurse can address through nursing interventions.
S — Signs and Symptoms (Defining Characteristics): The observable, measurable evidence that supports the diagnosis, introduced by the phrase "as evidenced by." These come directly from your assessment data.
The PES statement follows this template:
[Diagnostic Label] related to [Etiology] as evidenced by [Signs and Symptoms]
Example: Acute Pain related to surgical tissue trauma as evidenced by patient report of pain at 7 out of 10 on the Numeric Rating Scale, guarding behavior, elevated heart rate of 102 bpm, and facial grimacing.
Important exception: Risk diagnoses do not have an "as evidenced by" component because the problem has not yet occurred. They use "related to" only.
Example of a risk diagnosis: Risk for Falls related to impaired physical mobility, use of sedating medications, and age over 65.
How to Write Goals and Expected Outcomes
Goals and expected outcomes define what the patient will achieve as a result of nursing interventions. They must be patient-centered and written using the SMART framework.
SMART Goals:
S — Specific: States exactly what the patient will do
M — Measurable: Includes a measurable indicator (a number, a scale, or an observable behavior)
A — Achievable: Realistic given the patient's condition and available resources
R — Relevant: Directly relates to the nursing diagnosis
T — Time-bound: Includes a specific timeframe
Weak goal: "Patient will have less pain." This is not measurable, not time-bound, and not specific about what "less" means.
Strong goal: "Patient will report a pain level of 3 or below on the Numeric Rating Scale within 2 hours of analgesic administration." This is specific (pain level), measurable (NRS score of 3 or below), achievable (within the effect window of most analgesics), relevant (directly addresses the Acute Pain diagnosis), and time-bound (within 2 hours).
How to Write Nursing Interventions With Rationales
Each intervention in your care plan must have two parts: the specific nursing action and the evidence-based rationale explaining why that action addresses the diagnosis.
Weak intervention: "Monitor the patient." This is vague and has no rationale.
Strong intervention:
Intervention: Assess pain level using the Numeric Rating Scale every 2 hours and 30 minutes after analgesic administration.
Rationale: Regular pain assessment using a validated tool enables early identification of inadequate pain control and guides analgesic dose adjustments (ANA Standards of Professional Nursing Practice).
Your rationales should reference clinical guidelines, nursing textbooks, or peer-reviewed evidence where possible. This demonstrates that your interventions are evidence-based rather than arbitrary. When your care plan is part of an EBP assignment, the rationale section connects directly to the evidence you retrieved using your PICOT question. If you are unsure how to evaluate whether a source is appropriate for your rationale, the guide on identifying peer-reviewed sources covers five reliable methods.
Stuck on writing evidence-based rationales or choosing the right NANDA-I diagnosis? |
|---|
Writing a care plan that connects NANDA-I diagnostic labels to measurable SMART goals, backs every intervention with a specific evidence-based rationale, and evaluates outcomes against the nursing process framework requires both clinical knowledge and academic writing precision. ScribeLab Writer's nursing writing team supports nursing students with ADPIE-structured care plans, PES format diagnoses, and evidence-based rationales across all clinical scenarios. |
NIC, NOC, and the NNN Linkage
Three standardized nursing languages work together to structure care plans at an advanced level:
NANDA-I names the diagnosis. NIC (Nursing Interventions Classification) specifies the interventions. NOC (Nursing Outcomes Classification) defines the measurable outcomes.
NIC and NOC were developed at the University of Iowa College of Nursing and are, alongside NANDA-I, recognized by the ANA as standardized nursing languages. The NIC defines an intervention as "any treatment, based upon clinical judgment and knowledge, that a nurse performs to enhance patient/client outcomes" (Wagner et al., 2024).
The NNN framework links all three: NANDA-I names the problem, NIC specifies what the nurse does, and NOC measures the result.
Example linkage for Ineffective Airway Clearance:
NANDA-I Diagnosis: Ineffective Airway Clearance
NOC Outcome: Respiratory Status: Airway Patency (rated on a 5-point scale)
NIC Interventions: Airway Management, Cough Enhancement, Respiratory Monitoring
Most BSN programs require the basic ADPIE/PES structure. Some MSN programs and clinical documentation systems use the full NNN linkage. If your program requires NIC/NOC codes, reference the most recent NIC and NOC editions alongside the NANDA-I 13th edition.
10 Fully Worked Nursing Care Plan Examples
Each example below follows the complete ADPIE structure: Assessment Data, NANDA-I Diagnosis (PES format), Goals and Expected Outcomes, Nursing Interventions with Rationales, and Evaluation Criteria.
1. Acute Pain (Post-Surgical Patient)
Assessment data: 58-year-old male, day 1 post-open cholecystectomy. Reports pain at 7 out of 10 on the Numeric Rating Scale (NRS). Observed guarding of the abdominal incision site. Heart rate elevated at 102 bpm. Blood pressure 148/92 mmHg. Facial grimacing during movement.
Nursing diagnosis: Acute Pain related to surgical tissue trauma as evidenced by patient report of 7/10 on NRS, guarding behavior, heart rate of 102 bpm, blood pressure of 148/92, and facial grimacing during movement.
Goals and expected outcomes:
Patient will report pain at 3 or below on NRS within 2 hours of intervention (short-term)
Patient will demonstrate the use of at least one non-pharmacological pain management technique by the end of the shift (short-term)
Patient will report pain at 2 or below on NRS at rest by day 3 post-operatively (long-term)
Interventions and rationales:
Intervention: Administer prescribed analgesic (e.g., IV morphine or oral oxycodone) per physician order and reassess pain 30 minutes after administration. Rationale: Timely administration of prescribed analgesics targets pain pathways and reduces the physiological stress response. Reassessment at 30 minutes evaluates medication effectiveness within the expected onset window.
Intervention: Assess pain using the NRS every 2 hours and with each new report of pain. Rationale: Regular pain assessment using a validated tool allows early identification of inadequate pain control and provides objective data to guide analgesic adjustments.
Intervention: Assist the patient to reposition using pillow splinting over the incision during movement and coughing. Rationale: Splinting reduces strain on the surgical incision and decreases pain associated with movement, promoting participation in early mobilization, which is essential for post-operative recovery.
Intervention: Teach guided deep-breathing exercises and demonstrate their use. Rationale: Non-pharmacological pain management techniques such as deep breathing activate the parasympathetic nervous system, reduce muscle tension, and provide the patient with a self-management strategy for pain episodes between medication doses.
Evaluation criteria:
Goal met: Patient reports NRS of 3 or below within 2 hours.
Goal partially met: Patient reports NRS of 4 to 5 within 2 hours.
Goal not met: Patient reports NRS above 5 after intervention, requiring reassessment and revision of the plan.
2. Impaired Physical Mobility (Post-Hip Replacement)
Assessment data: 72-year-old female, day 2 post-total hip replacement. Unable to ambulate independently. Requires assistance for bed-to-chair transfer. Limited range of motion in the right hip. Reports fear of falling. Uses a walker.
Nursing diagnosis: Impaired Physical Mobility related to musculoskeletal impairment secondary to hip replacement surgery as evidenced by inability to ambulate independently, limited range of motion in the right hip, and requirement for an assistive device.
Goals and expected outcomes:
Patient will ambulate 50 feet with a walker and standby assistance within 48 hours (short-term)
Patient will perform bed-to-chair transfers with minimal assistance within 72 hours (short-term)
Patient will ambulate independently with a walker by discharge (long-term)
Interventions and rationales:
Intervention: Assist with progressive ambulation three times daily, beginning with 25 feet and increasing to 50 feet as tolerated. Rationale: Progressive ambulation prevents complications of immobility (deep vein thrombosis, pneumonia, pressure injuries), promotes muscle strength, and restores functional independence within safe parameters.
Intervention: Coordinate with physical therapy for daily range-of-motion exercises and gait training. Rationale: Physical therapists provide specialized expertise in post-surgical mobility rehabilitation and prescribe exercises that safely increase the range of motion while protecting the surgical site.
Intervention: Assess and address the patient's fear of falling through education on fall prevention strategies and demonstration of safe transfer techniques. Rationale: Fear of falling is a documented barrier to post-surgical mobility. Patient education reduces anxiety and promotes confidence in safe movement.
Intervention: Ensure the call bell is within reach at all times and the bed is in the lowest position with side rails up as appropriate. Rationale: Environmental safety measures reduce the risk of falls during the period of impaired mobility.
Evaluation criteria:
Goal met: Patient ambulates 50 feet with walker and standby assistance within 48 hours.
Goal partially met: Patient ambulates 25 feet but requires physical assistance beyond standby.
Goal not met: Patient is unable to ambulate, requiring reassessment of pain control, fear, or physical barriers
3. Risk for Falls (Elderly Patient)
Assessment data: 78-year-old male admitted for pneumonia treatment. History of two falls at home in the past 3 months. Morse Fall Scale score of 55 (high risk). Currently on IV antibiotics and receives a sedating cough suppressant at night. Uses eyeglasses for distance vision. Unsteady gait observed on admission.
Nursing diagnosis: Risk for Falls related to unsteady gait, history of falls, advanced age, sedating medication use, and impaired visual acuity.
Goals and expected outcomes:
Patient will remain free from falls during the hospital stay (ongoing)
Patient will demonstrate safe use of the call bell and request assistance before ambulating within 24 hours (short-term)
Interventions and rationales:
Intervention: Implement fall precautions per hospital protocol: yellow fall-risk wristband, bed alarm, non-slip socks, and room close to the nursing station. Rationale: Standardized fall precautions alert all staff to the patient's risk level and provide environmental modifications that reduce the likelihood of a fall event.
Intervention: Reassess fall risk using the Morse Fall Scale every shift and after any change in medication or condition. Rationale: Ongoing assessment identifies changes in risk status and allows timely adjustment of precautions, particularly when sedating medications are added or doses are changed.
Intervention: Educate the patient and family on fall prevention: use of the call bell before getting out of bed, keeping eyeglasses within reach, and wearing non-slip footwear. Rationale: Patient and family education promotes active participation in fall prevention and ensures safety measures continue when nursing staff is not in the room.
Intervention: Conduct hourly rounding to assess patient needs (toileting, pain, repositioning) and reduce the likelihood of the patient attempting to get up unassisted. Rationale: Proactive hourly rounding has been associated with reduced fall rates in hospitalized patients because it addresses the common reasons patients attempt to ambulate without assistance.
Evaluation criteria:
Goal met: No fall events during hospitalization.
Goal not met: Fall occurs, requiring incident documentation, post-fall assessment, and care plan revision.
4. Ineffective Airway Clearance (Pneumonia Patient)
Assessment data: 65-year-old male with community-acquired pneumonia. Productive cough with thick yellow sputum. Oxygen saturation 91% on room air. Respiratory rate 24 breaths per minute. Diminished breath sounds in the right lower lobe on auscultation. Temperature 38.6 degrees Celsius.
Nursing diagnosis: Ineffective Airway Clearance related to excessive mucus production and infection as evidenced by productive cough with thick yellow sputum, oxygen saturation of 91% on room air, respiratory rate of 24, and diminished breath sounds in the right lower lobe.
Goals and expected outcomes:
Patient will maintain oxygen saturation above 94% within 4 hours (short-term)
Patient will demonstrate an effective coughing technique within 24 hours (short-term)
Patient will have clear or diminished adventitious breath sounds by day 3 (long-term)
Interventions and rationales:
Intervention: Elevate the head of the bed to 30 to 45 degrees. Rationale: Semi-Fowler's position promotes diaphragmatic descent and lung expansion, improving ventilation and facilitating drainage of secretions from the affected lobe.
Intervention: Encourage fluid intake of 2 to 3 liters per day unless contraindicated. Rationale: Adequate hydration thins mucus secretions, making them easier to expectorate and reducing the risk of mucus plugging.
Intervention: Teach and encourage the use of incentive spirometry every 1 to 2 hours while awake. Rationale: Incentive spirometry promotes deep breathing, prevents atelectasis, and aids in mobilizing secretions from the lower airways.
Intervention: Monitor oxygen saturation continuously and administer supplemental oxygen as prescribed to maintain SpO2 above 94%. Rationale: Continuous pulse oximetry provides objective data on gas exchange and guides supplemental oxygen therapy to prevent hypoxemia.
Evaluation criteria:
Goal met: SpO2 above 94% within 4 hours, effective coughing demonstrated within 24 hours.
Goal partially met: SpO2 improves to 93% but remains below target.
Goal not met: SpO2 remains below 92%, requiring escalation of respiratory support.
5. Imbalanced Nutrition: Less Than Body Requirements (Oncology Patient)
Assessment data: 45-year-old female undergoing chemotherapy for breast cancer. Reports persistent nausea, loss of appetite, and difficulty eating for the past 2 weeks. Weight loss of 4 kg in 3 weeks. BMI 17.8 (underweight). Serum albumin 2.8 g/dL (low). Reports eating less than 50% of meals served.
Nursing diagnosis: Imbalanced Nutrition: Less Than Body Requirements related to chemotherapy-induced nausea and anorexia as evidenced by weight loss of 4 kg in 3 weeks, BMI of 17.8, serum albumin of 2.8 g/dL, and intake of less than 50% of meals.
Goals and expected outcomes:
Patient will consume at least 75% of meals within 48 hours (short-term)
Patient will maintain current body weight with no further loss within 1 week (short-term)
Patient will achieve serum albumin of 3.5 g/dL or above within 4 weeks (long-term)
Interventions and rationales:
Intervention: Administer prescribed antiemetics 30 minutes before meals. Rationale: Prophylactic antiemetic administration reduces chemotherapy-induced nausea before eating, increasing the likelihood that the patient can tolerate and retain oral intake.
Intervention: Offer small, frequent meals (six per day) with high-protein, high-calorie options based on patient preferences. Rationale: Small, frequent meals are better tolerated than three large meals in patients experiencing nausea. High-protein, high-calorie foods maximize nutritional value per serving.
Intervention: Weigh the patient every morning before breakfast using the same scale and clothing. Rationale: Consistent daily weights provide accurate trending data to evaluate whether nutritional interventions are preventing further weight loss.
Intervention: Request a dietitian consultation for individualized nutritional assessment and meal planning. Rationale: Registered dietitians provide specialized expertise in oncology nutrition and can recommend supplements, fortified foods, or enteral nutrition if oral intake remains inadequate.
Evaluation criteria:
Goal met: Consuming 75% or more of meals within 48 hours, weight stabilized within 1 week.
Goal partially met: Consuming 50 to 74% of meals, weight loss slowed but not stabilized.
Goal not met: Intake remains below 50%, weight continues to decline, requiring escalation to enteral nutrition assessment
6. Anxiety Related to Surgical Procedure
Assessment data: 34-year-old female, pre-operative for elective laparoscopic hysterectomy scheduled for the following morning. Reports feeling "very anxious" and "unable to stop thinking about what could go wrong." Heart rate 98 bpm. Blood pressure 140/88 mmHg. Observed restlessness, hand wringing, and difficulty maintaining eye contact. Reports sleeping only 2 hours the previous night.
Nursing diagnosis: Anxiety related to upcoming surgical procedure and fear of complications as evidenced by patient statement of being "very anxious," heart rate of 98 bpm, blood pressure of 140/88, restlessness, hand wringing, and insomnia (2 hours of sleep).
Goals and expected outcomes:
Patient will verbalize an understanding of the surgical procedure and expected recovery within 4 hours (short-term)
Patient will report reduced anxiety using a self-rated anxiety scale (0 to 10) from the current level to 4 or below by bedtime (short-term)
Patient will demonstrate at least one relaxation technique before surgery (short-term)
Interventions and rationales:
Intervention: Provide pre-operative education about the procedure, expected recovery timeline, and post-operative pain management plan in clear, non-medical language. Rationale: Knowledge deficit is a common contributor to pre-operative anxiety. Patient education reduces the fear of the unknown and allows the patient to develop realistic expectations.
Intervention: Allow the patient to ask questions and express concerns without interruption. Rationale: Active listening and therapeutic communication validate the patient's feelings and establish trust, which reduces anxiety.
Intervention: Teach and guide the patient through a progressive muscle relaxation exercise. Rationale: Progressive muscle relaxation activates the parasympathetic nervous system, reducing physiological markers of anxiety (heart rate, blood pressure) and providing the patient with a tool for self-management.
Intervention: Minimize environmental stressors: reduce noise, dim lights, and limit unnecessary interruptions during the evening. Rationale: A calm environment supports relaxation and promotes sleep, which is essential for physiological and psychological readiness for surgery.
Evaluation criteria:
Goal met: Patient verbalizes understanding of the procedure, reports anxiety at 4 or below, and demonstrates a relaxation technique.
Goal partially met: Patient reports reduced anxiety but remains above 4, or is unable to demonstrate a relaxation technique.
Goal not met: Anxiety worsens, or the patient is unable to sleep, requiring reassessment and possible pharmacological intervention
7. Risk for Pressure Injury (Immobile ICU Patient)
Assessment data: 81-year-old male, intubated and sedated in the ICU for 3 days following emergency abdominal surgery. Braden Scale score of 11 (high risk). Unable to reposition independently. Incontinence managed with an indwelling urinary catheter. Nutritional status poor (serum albumin 2.5 g/dL). Skin intact on admission, but with non-blanchable erythema observed on the sacrum.
Nursing diagnosis: Risk for Pressure Injury related to immobility, poor nutritional status, advanced age, and moisture exposure from incontinence.
Goals and expected outcomes:
Patient will maintain skin integrity with no progression from erythema to tissue breakdown throughout the ICU stay (ongoing)
Non-blanchable erythema on the sacrum will resolve within 72 hours (short-term)
Interventions and rationales:
Intervention: Reposition the patient every 2 hours using a turning schedule documented on the bedside chart. Rationale: Repositioning redistributes pressure across body surfaces and prevents sustained pressure on bony prominences, which is the primary cause of pressure injuries.
Intervention: Apply a pressure-relieving mattress (alternating pressure or low-air-loss) and use foam heel elevation devices. Rationale: Pressure redistribution surfaces reduce interface pressure below capillary closing pressure, maintaining tissue perfusion in patients who cannot reposition independently.
Intervention: Conduct a full skin assessment every shift with documentation of any changes in the sacral erythema. Rationale: Early detection of skin changes enables prompt intervention before tissue breakdown progresses to a Stage 2 or higher pressure injury.
Intervention: Optimize nutritional intake through collaboration with the dietitian to increase protein and caloric delivery. Rationale: Adequate protein intake supports tissue integrity and wound healing. Serum albumin below 3.0 g/dL is an independent risk factor for pressure injury development.
Evaluation criteria:
Goal met: Skin integrity maintained, sacral erythema resolves within 72 hours.
Goal partially met: No new skin breakdown, but erythema persists beyond 72 hours.
Goal not met: Pressure injury develops, requiring wound care consultation and care plan revision.
8. Deficient Knowledge (Newly Diagnosed Type 2 Diabetes)
Assessment data: 52-year-old male, newly diagnosed with type 2 diabetes. No prior experience with blood glucose monitoring. Prescribed metformin 500 mg twice daily and a diabetic diet. Unable to describe the purpose of metformin or how to check blood glucose when asked. Reports confusion about dietary modifications. HbA1c of 8.2%.
Nursing diagnosis: Deficient Knowledge related to newly diagnosed type 2 diabetes as evidenced by inability to describe medication purpose, inability to demonstrate blood glucose monitoring, and verbalized confusion about dietary modifications.
Goals and expected outcomes:
Patient will correctly demonstrate blood glucose self-monitoring within 24 hours (short-term)
Patient will verbalize the purpose, dose, and timing of metformin within 24 hours (short-term)
Patient will identify three foods to limit and three foods to increase for blood glucose management within 48 hours (short-term)
Patient will maintain a blood glucose log and bring it to the first outpatient follow-up appointment (long-term)
Interventions and rationales:
Intervention: Provide one-on-one diabetes self-management education using the teach-back method, covering blood glucose monitoring technique, metformin purpose and timing, and basic dietary principles. Rationale: Individualized education with teach-back ensures the patient can demonstrate skills and knowledge rather than simply receiving information. Teach-back is recommended by the Agency for Healthcare Research and Quality (AHRQ) as a best practice for health literacy. For nursing students writing an EBP paper alongside a care plan assignment, a nursing annotated bibliography is the standard method for documenting the evidence base for these kinds of educational interventions.
Intervention: Demonstrate blood glucose self-monitoring step by step and have the patient return to demonstrate. Rationale: Psychomotor skills such as glucometer use require hands-on practice and return demonstration to confirm competence before discharge.
Intervention: Provide written educational materials at an appropriate literacy level, including a blood glucose log template. Rationale: Written materials reinforce verbal education and serve as a reference for the patient at home when the nurse is not available to answer questions.
Intervention: Request a certified diabetes educator (CDE) or dietitian consultation for comprehensive dietary counseling. Rationale: CDEs and dietitians provide specialized, individualized nutritional guidance that extends beyond what can be covered in a single nursing education session.
Evaluation criteria:
Goal met: Patient correctly demonstrates glucose monitoring, verbalizes medication purpose, and identifies appropriate foods.
Goal partially met: Patient demonstrates one or two skills but requires additional reinforcement on others.
Goal not met: Patient unable to demonstrate or verbalize core knowledge, requiring repeat education sessions before discharge.
9. Ineffective Breathing Pattern (COPD Exacerbation)
Assessment data: 68-year-old female admitted with acute exacerbation of chronic obstructive pulmonary disease (COPD). Respiratory rate 28 breaths per minute. Uses accessory muscles during breathing. Oxygen saturation 89% on room air. Pursed-lip breathing was observed intermittently. Reports dyspnea at rest. ABG results show pH 7.33, PaCO2 52 mmHg, PaO2 58 mmHg.
Nursing diagnosis: Ineffective Breathing Pattern related to airway obstruction and COPD exacerbation as evidenced by respiratory rate of 28, use of accessory muscles, oxygen saturation of 89%, dyspnea at rest, and ABG showing respiratory acidosis (pH 7.33, PaCO2 52).
Goals and expected outcomes:
Patient will achieve oxygen saturation of 90 to 92% (COPD target range) within 2 hours (short-term)
Patient will report reduced dyspnea using a modified Borg scale within 4 hours (short-term)
Patient will demonstrate effective pursed-lip and diaphragmatic breathing within 24 hours (short-term)
Interventions and rationales:
Intervention: Administer supplemental oxygen via nasal cannula at 1 to 2 liters per minute as prescribed, titrating to maintain SpO2 between 88 and 92%. Rationale: In COPD patients, the hypoxic drive may be the primary stimulus for respiration. High-flow oxygen can suppress this drive and worsen CO2 retention. Target saturation for COPD is 88 to 92%, not the standard 94 to 98%.
Intervention: Position the patient in high Fowler's or tripod position. Rationale: Upright positioning maximizes diaphragmatic excursion and reduces the work of breathing by allowing gravity to assist lung expansion.
Intervention: Teach and reinforce pursed-lip breathing and diaphragmatic breathing techniques. Rationale: Pursed-lip breathing creates back-pressure in the airways, preventing premature airway collapse and improving gas exchange. Diaphragmatic breathing reduces the reliance on accessory muscles and improves breathing efficiency.
Intervention: Monitor ABG results as ordered and report worsening respiratory acidosis to the physician. Rationale: Serial ABG monitoring provides objective data on the patient's acid-base status and guides adjustments to respiratory support, including the need for non-invasive ventilation.
Evaluation criteria:
Goal met: SpO2 between 90 and 92%, reduced dyspnea on the Borg scale, demonstrates breathing techniques.
Goal partially met: SpO2 improves but remains below 90%, or dyspnea persists.
Goal not met: SpO2 below 88% or PaCO2 continues to rise, requiring escalation to BiPAP or intubation
10. Deficient Fluid Volume (Dehydration)
Assessment data: 26-year-old female admitted with acute gastroenteritis. Reports vomiting 8 times and watery diarrhea 6 times in the past 24 hours. Oral intake minimal. Heart rate 110 bpm. Blood pressure 96/62 mmHg. Skin turgor decreased (tenting over the sternum). Mucous membranes dry. Urine output 20 mL per hour (below the normal minimum of 30 mL per hour). BUN 28 mg/dL (elevated). Specific gravity 1.035 (concentrated).
Nursing diagnosis: Deficient Fluid Volume related to excessive gastrointestinal losses from vomiting and diarrhea as evidenced by heart rate of 110 bpm, blood pressure of 96/62, decreased skin turgor, dry mucous membranes, urine output of 20 mL/hr, BUN of 28 mg/dL, and urine specific gravity of 1.035.
Goals and expected outcomes:
Patient will have urine output of 30 mL per hour or greater within 4 hours (short-term)
Patient will demonstrate improved skin turgor and moist mucous membranes within 8 hours (short-term)
Patient will maintain heart rate below 100 bpm and blood pressure above 100/60 within 6 hours (short-term)
Patient will tolerate oral fluids without vomiting within 24 hours (long-term)
Interventions and rationales:
Intervention: Initiate IV fluid resuscitation as prescribed (e.g., 0.9% normal saline at 150 to 200 mL/hr for the first 2 hours, then reassess). Rationale: Isotonic IV fluids replace extracellular fluid losses and restore circulating volume. The initial bolus rate is guided by the degree of dehydration and hemodynamic instability.
Intervention: Monitor intake and output strictly, including emesis and diarrheal output, every hour. Rationale: Accurate I and O tracking quantifies ongoing losses and evaluates whether IV replacement is adequate to achieve positive fluid balance.
Intervention: Assess vital signs every 2 hours, including heart rate, blood pressure, and orthostatic changes. Rationale: Tachycardia and hypotension are early indicators of hypovolemia. Trending vital signs provides objective evidence of fluid status improvement or deterioration.
Intervention: Administer prescribed antiemetics before attempting oral rehydration with small, frequent sips of clear fluids. Rationale: Controlling nausea and vomiting before introducing oral fluids increases the likelihood of tolerance and supports the transition from IV to oral hydration.
Evaluation criteria:
Goal met: Urine output above 30 mL/hr, skin turgor improved, vital signs within target ranges, tolerating oral fluids.
Goal partially met: Urine output improving but below 30 mL/hr, vital signs trending toward normal.
Goal not met: Urine output remains below 20 mL/hr or vital signs worsen, requiring fluid bolus reassessment and possible escalation. How Care Plans Differ Across Nursing Education Systems.
The care plan is taught in nursing programs worldwide, but the specific frameworks and terminology vary.
United States: BSN programs emphasize NANDA-I diagnoses, PES format, and the ADPIE framework. The AACN Essentials (2021) embed clinical reasoning and patient-centered care across all 10 domains of professional nursing education. Care plans are formally graded assignments in most BSN curricula and are assessed during the NCLEX-RN licensure examination.
United Kingdom: The NMC Standards of Proficiency for Registered Nurses (2018) require that nurses demonstrate person-centered care planning. UK programs often use nursing models such as the Roper-Logan-Tierney Activities of Living Model rather than NANDA-I. Care plans may be framed around activities of daily living rather than standardized diagnostic labels.
Australia: The NMBA Registered Nurse Standards for Practice (2016) require evidence-based care planning. Australian nursing programs use a mix of NANDA-I and locally developed frameworks. Many Australian universities follow a format similar to the US approach.
Saudi Arabia and UAE: Nursing programs accredited by the Saudi Commission for Health Specialties (SCFHS) and UAE regulatory bodies increasingly follow US-style NANDA-I and ADPIE frameworks, particularly at institutions aligned with US accreditation standards.
South Africa and Nigeria: The South African Nursing Council (SANC) and the Nursing and Midwifery Council of Nigeria (NMCN) regulate nursing education. Care plan requirements follow institutional standards, with many research-active programs adopting NANDA-I and the nursing process model.
You May Also Find Useful
Common Nursing Care Plan Mistakes
Writing a Medical Diagnosis Instead of a Nursing Diagnosis
"Pneumonia" is a medical diagnosis. "Ineffective Airway Clearance related to excessive mucus production as evidenced by productive cough and diminished breath sounds" is a nursing diagnosis. The medical diagnosis belongs in the patient history, not in the nursing diagnosis statement.
Goals That Are Not Measurable
"Patient will feel better" is not measurable. "Patient will report pain at 3 or below on the NRS within 2 hours." Every goal needs a number, a scale, a behavior, or a timeframe that allows you to determine whether it was met objectively.
Interventions Without Rationales
Listing what you will do without explaining why is incomplete. Every intervention needs a rationale that connects the nursing action to the patient outcome. "Elevate the head of the bed" is an instruction. "Elevate the head of the bed to 30 degrees to promote lung expansion and facilitate drainage of secretions" is an intervention with a rationale.
Skipping the Evaluation
The evaluation is not optional. It completes the nursing process cycle. If a goal was not met, the evaluation should state what was observed and what the revised plan will be. Leaving the evaluation blank or writing "will continue to monitor" without specifics is the most common reason care plans are returned for revision.
Using Vague Assessment Data
"Patient is in pain" is subjective and vague. "Patient reports pain at 7/10 on the NRS, with observed guarding and elevated heart rate of 102 bpm" is objective, specific, and directly supports the nursing diagnosis. Your assessment data is the evidence that justifies every decision in the care plan.
A Care Plan Checklist Before You Submit
Before submitting your care plan assignment, check it against this list:
Assessment data includes both subjective and objective findings.
The nursing diagnosis is in PES format (or risk format for risk diagnoses)
The diagnosis is a nursing diagnosis, not a medical diagnosis.
All goals are SMART: Specific, Measurable, Achievable, Relevant, Time-bound.
Every intervention has a specific nursing action and an evidence-based rationale.
Interventions are within the scope of nursing practice (not medical orders)
The evaluation states whether each goal was met, partially met, or not met.
If a goal was not met, the evaluation includes a plan for reassessment and revision.
The care plan uses current NANDA-I terminology from the 13th edition (2024 to 2026)
All sources are cited in APA 7th edition format
Frequently Asked Questions About Nursing Care Plans
What is the difference between a medical diagnosis and a nursing diagnosis?
A medical diagnosis identifies a disease or pathological condition and is made by a physician. A nursing diagnosis identifies the patient's response to an actual or potential health problem and is made by a registered nurse. The medical diagnosis is relatively static until the disease is treated. The nursing diagnosis changes as the patient's condition and responses change. For example, "heart failure" is a medical diagnosis. "Activity intolerance related to imbalance between oxygen supply and demand as evidenced by dyspnea on exertion and fatigue with minimal activity" is a nursing diagnosis.
What is the PES format?
PES stands for Problem, Etiology, and Signs/Symptoms. It is the standard format for writing a NANDA-I nursing diagnosis statement. The Problem is the diagnostic label, the Etiology is introduced by "related to," and the Signs/Symptoms are introduced by "as evidenced by." Risk diagnoses do not include the "as evidenced by" component.
How many nursing diagnoses should a care plan have?
Most BSN programs require two to four nursing diagnoses per care plan, prioritized using Maslow's hierarchy of needs. Physiological needs (airway, breathing, circulation, pain) are addressed first, followed by safety needs, then psychosocial needs. Your instructor will specify the expected number.
What is the difference between a goal and an expected outcome?
In many nursing programs, goals and expected outcomes are used interchangeably. When they are distinguished, a goal is a broader statement of desired improvement (e.g., "patient will achieve adequate pain control"), and an expected outcome is the specific, measurable indicator of that goal (e.g., "patient will report pain at 3 or below on NRS within 2 hours"). Always write specific, measurable outcomes regardless of which term your program uses.
Do I need to use NIC and NOC codes?
Most BSN-level care plans do not require NIC and NOC codes. They require NANDA-I diagnoses, individualized interventions with rationales, and SMART goals. NIC and NOC are more commonly used in MSN programs, electronic health record documentation, and clinical practice settings that use the full NNN framework. Check your assignment guidelines.
How current should my sources be?
For nursing care plan assignments, use sources from the last 5 to 7 years wherever possible. The NANDA-I reference should be the current edition (13th edition, 2024 to 2026). Foundational sources such as the ANA Standards or established nursing textbooks like Ackley and Ladwig's Nursing Diagnosis Handbook are acceptable regardless of age.
Can I use the same care plan format for different patients?
The ADPIE format remains the same, but every care plan must be individualized to the specific patient. The assessment data, diagnosis, goals, and interventions should reflect that particular patient's condition, history, and preferences. Submitting a generic or template care plan without patient-specific details is the most common reason for low marks.
Putting the Care Plan Into Practice
The nursing care plan is where clinical reasoning becomes visible. It is the document that demonstrates you can look at a patient, identify what the nursing priorities are, connect those priorities to evidence-based interventions, and evaluate whether your actions made a difference.
The 10 examples in this guide cover the most common clinical scenarios you will encounter in nursing school. The format is the same for all of them: assess, diagnose, plan, implement, evaluate. Master the format with these examples, then apply it to any patient scenario your instructor gives you.
If you are working on a nursing care plan assignment and need support with the NANDA-I diagnosis, APA formatting, or evidence-based rationales, ScribeLab Writer's nursing writing service works with BSN and MSN students across the US, UK, Australia, and internationally.
